



Contents
Scroll to:
https://doi.org/10.17749/2077-8333/epi.par.con.2023.148
Scroll to:
Objective: to investigate sexual disorders (SDs) in patients with temporal lobe epilepsy (TLE) both before and after undergoing various temporal lobe operative procedures.
Material and methods. A retrospective andrological and sexologic study was conducted, utilizing catamnesis data. Multiple examination methods were employed, including semen and prostatic fluid analysis, Decourt–Dumic sperm morphotype analysis, vegetative tests, Shcherbak thermoregulation reflex examination, ultraviolet erythema test, sugar curve analysis, and electroencephalography. The study assessed the results of surgical treatment and long-term catamnesis for 120 TLE patients who had undergone various temporal lobe operative procedures (TLPs), with ages at the time of surgery ranging from 4.5 to 47 years. Among them, 82 patients (41 males and 41 females) in the main group reported complaints of SDs, representing 100% for all calculations.
Results. Hypersexuality and sexual perversions were most prevalent among patients with severe mental disorders. Following TLPs, patients with mild mental disorders and cessation of epileptic seizures (EPs) experienced regression in 83.6% of SD cases. Conversely, among patients with severe mental disorders, SDs regressed in 45% of cases after TLPs. Encouraging outcomes were observed in patients with hypersexuality, which was ameliorated after the cessation of EPs, with a catamnesis period ranging from 17 to 24 years.
Conclusion. This study, conducted in real-world clinical settings, supports the recommendation of surgical treatment for TLE patients with mild mental disorders. In the majority of cases, the cessation or reduction of EPs following TLPs leads to improvements in TLE manifestations, including the patient's mental state, SDs, and social adaptation.
Shefer D.G., Shershever A.S., Boreyko V.B., Klein A.V., Sorokova E.V. Sexual disorders among temporal lobe epilepsy patients preand post-surgery. Epilepsy and paroxysmal conditions. 2023;15(3):210–221. https://doi.org/10.17749/2077-8333/epi.par.con.2023.148
Sexual dysfunctions in patients with temporal lobe epilepsy (TLE) have been extensively documented by numerous researchers in clinical studies, and these findings have been also substantiated by experimental studies [1–6]. A noteworthy observation was made by A.E. Wolker (1957) [3], who highlighted that many individuals with TLE often report experiencing sexual disorders (SDs) that, from the patient's perspective, may hold more significance than the actual epileptic seizures (ES). The author discussed a group of 50 TLE patients, of which 29 exhibited severe hyposexuality prior to surgery, characterized by a complete absence of sexual desire and orgasm. Following surgery on the mediobasal structures of the temporal region, a third of the operated patients showed an increase in sexual activity alongside ES cessation [3]. H. Gastaut et al. (1955) were pioneers in describing profound apathy towards sexual activity (global hyposexuality) in TLE patients, some of whom were oblivious to this sexual deficit. This could be attributed to the absence of any sexual drive throughout their lives or, in some cases, the nascent sexuality would swiftly fade following the onset of ES [6]. These authors also documented a case of exhibitionism as a manifestation of a psychomotor seizure.
Since the experimental study by H. Kluver and P. Bucy (1938) [7], which induced hypersexuality in adult animals through bilateral temporal lobectomy, a substantial body of clinical and experimental evidence has been amassed, overwhelmingly establishing the involvement of limbic brain structures in the genesis of hypersexuality [8–11]. For instance, C.D. Wood (1958) [11] observed hypersexuality when the lateral temporal lobe was compromised, while J. Pilleri (1966) [8] noted heightened sexuality alongside oral behaviors and reduced emotionality during bilateral temporal lobectomy. P.D. Maclean (1954 and 1955) observed penile erection in monkeys following electrical stimulation of the precingulate gyrus [1][12].
Certain experimental studies have provided insights into the fluctuations in sexual activity associated with temporal lobe pathology [13]. For example, after amygdalectomy, cats exhibit tamer and hypersexual behavior, but subsequent destruction of the ventromedial nuclei of the hypothalamus transforms them into aggressive hyposexual animals. These studies collectively emphasize that pathological conditions affecting brain limbic system can indeed lead to disruptions in sexual function [14–16].
SDs can manifest in various brain diseases, such as tumors, brain injuries, and others [17]. The testes, known for their significant role as endocrine glands in men, actively contribute to the expression of sexual functions. It's established that there are close functional connections between the testes and the limbic-pituitary complex. Any alterations within this system, whether functional-dynamic or organic, might likely result in morphological changes in the testes. Surprisingly, there's a gap in the literature concerning the testicular structure of TLE patients. Researchers investigating SDs consistently report significant challenges when attempting to gather a "sexual history" due to patients' reluctance or hesitation in disclosing intimate aspects of their lives. Furthermore, in cases where epilepsy develops in the early years of life, "sexual infantilism" is frequently observed, and some individuals surveyed might not have reached puberty yet.
In our own clinical practice, we have faced these same challenges when collecting a "sexual history." As a result, we present subjective data that reflect SDs in our patients.
Objective: to investigate SDs in TLE patients both before and after undergoing various temporal lobe operative procedures.
We conducted a comprehensive examination of the outcomes following surgical treatment and long-term monitoring of 120 TLE patients who underwent various surgical interventions on the temporal lobe, and among them, 82 patients reported experiencing SDs. Consequently, we selected these 82 patients (41 males and 41 females) for detailed analysis. The follow-up of these patients was halted in 2004, and the follow-up data were meticulously evaluated within the period of 2020–2022.
The duration of the catamnesis (medical history review) ranged from 17 to 24 years (±6 years). The age of patients at the time of surgery ranged from 4.5–47 years. As indicated in Table 1, almost one-third of the patients underwent surgery during the age range of 10–19 years. Surgical intervention was performed in only 1 patient under the age of 5.
Table 1. Patients with temporal lobe epilepsy and complaints of sexual disorders stratified by age at the time of surgery
Таблица 1. Распределение больных височной эпилепсией с жалобами на сексуальные нарушения по возрасту к моменту операции
|
Patient age at surgery / Возраст в момент операции |
Number of patients, n (%) / Число больных, n (%) |
|
1–5 years / 1–5 лет |
1 (1,2) |
|
6–10 years / 6–10 лет |
4 (4,8) |
|
11–15 years / 11–15 лет |
20 (24,3) |
|
16–20 years / 16–20 лет |
13 (15,8) |
|
21–25 years / 21–25 лет |
14 (17,1) |
|
26–30 years / 26–30 лет |
7 (8,5) |
|
31–35 years / 31–35 лет |
13 (15,8) |
|
36–40 years / 36–40 лет |
10 (12,3) |
|
Total / Всего |
82 (100,0) |
All patients included in our analysis were individuals with TLE who reported complaints of SDs before undergoing surgical treatment. These patients were subsequently divided into two groups: Group 1 (n=49) consisted of patients with minor mental disorders, while Group 2 (n=33) comprised individuals with severe mental disorders.
To assess the patients, we employed specialized examination techniques, which included the analysis of sperm and prostatic fluid, as well as the determination of morphotypes using the Decourt–Dumic method. Additionally, unilateral testicular excision biopsies were conducted in 23 patients, with 3 individuals aged between ≥25 and <30, and 20 individuals aged between ≥30 and <35. The biopsied fragments were subjected to thorough histological and histochemical scrutiny. Hematoxylin and eosin, microfuxin, and Van Gieson staining were used in this process, followed by optical microscopy with ×140 magnification.
A comprehensive study was conducted, which included neurological and neuropsychological examinations. To further understand the nature of brain involvement, all patients underwent pneumoencephalography [18].
Electroencephalography (EEG) was performed using surface electrodes positioned according to the international "10–20" system. This was carried out on the Alvar encephalograph (France) as well as the multifunctional neurophysiological system Nicolet, using the Bravo program (Nicolet Biomedical, USA).
The assessment of work capacity for adults was based on the following criteria:
For children and adolescents, the evaluation criteria were as follows:
In terms of legal procedures, patients or their relatives completed informed voluntary consent forms for all medical interventions. The study adhered to the principles outlined in the Helsinki Declaration of the World Medical Association. Given that the data extracted from medical records for analysis within the scope of this retrospective follow-up study were provided in a de-identified (anonymous) manner, it was not required to have patients sign an informed consent form specifically for participation in the study.
This paper presents information regarding the distribution of characteristics within two groups of TLE patients with comorbid psychiatric disorders. The analysis encompasses both quantitative and qualitative features. Quantitative features encompass the frequency of epileptic seizures and the duration of the disease prior to surgical intervention. Qualitative features include the use of instrumental research methods, the specific type of surgical intervention employed, outcomes from histological examination, and the overall surgical outcomes.
In Group 1 (n=49), the following mental disorders were identified: mild memory impairment for current events, affective fluctuations primarily within the context of dysthymia, and initial personality changes resembling epileptic traits. Some patients experienced short-term postseizure twilight states of consciousness, with no impact on their overall intelligence.
Patients in Group 1 were characterized by a lifelong absence of sexual desire. Interestingly, these individuals did not perceive this lack of sexual desire as distressing, as they were not conscious of their defect, displaying complete indifference to matters of gender. Patients in this group exhibited symptoms of organic cerebral pathology resulting from birth-related cranial trauma or early childhood nervous system infections, leading to delayed puberty. They also had a history of intolerance to heat, stuffiness, changes in atmospheric pressure, allergies to food and medications, nosebleeds, nighttime urinary incontinence, and later (after 23 years) the appearance of nocturnal emissions.
Objective examinations revealed signs of feminization, pseudocryptorchidism, and other indicators suggesting a delay in both sexual and physical development. It was noted that all patients in this group had the involvement of hypothalamic nuclei in the pathological process, in addition to the temporal structures. This was confirmed by specific complaints which required objective assess- ments and additional tests (vegetative tests, Shcherbak thermoregulatory reflex, ultraviolet erythema test, EEG results, blood glucose fluctuations, etc.). Following the surgical intervention, patients in Group 1 continued to experience persistent global hyposexuality.
It was crucial to investigate whether the observed global hyposexuality was solely dependent on the processes occurring in the mediobasal parts of the temporal region, which involves the hypothalamic nuclei and other structures of the limbic system, or if it also had an impact on the functioning of certain endocrine glands, primarily the testes, in the pathogenic chain of SDs. This inquiry gains importance considering the intimate functional connections between limbic and hypothalamic structures, along with the secondary involvement of hypothalamic formations due to pathological influence originating from the limbic region [2][19][20].
To address this question, we conducted testicular biopsies on 17 patients from Group 1 aged 21 to 30, following established indications [4]. Morphological analysis of the testicular tissue revealed a correlation between the depth of testicular lesion and the degree of involvement of the hypothalamic nuclei in the pathological process. Specifically, the more extensive the involvement of the hypothalamic region, the more pronounced the observed histological alterations in the testis.
In these patients, the seminiferous tubules displayed incomplete spermatogenesis. Some individuals exhibited only Sertoli cells within their tubules, while others showed spermatogenic elements (spermatogonia, spermatocytes), and 1 patient had spermatids. Notably, spermatogenesis in these patients terminated at the meiosis stage, and spermiogenesis did not occur as expected. Significant changes were evident in the interstitial tissue. A marked reduction in the number of Leydig cells with accompanying degenerative features was observed in the testes of all patients in this group, indicating the central origin of these disorders (Fig. 1).
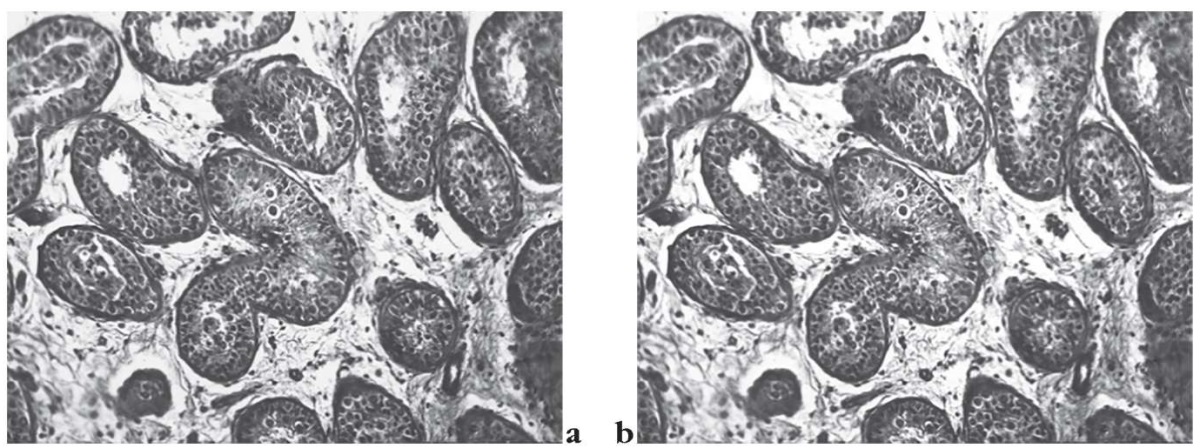
Figure 1. Light microscopy (stained with hematoxylin
and eosin, microfuxin, Van Gieson stain, magnification ×140;
the assay was performed by pathomorphologist A.V. Klein, MD, PhD).
Testis morphology is drastically changed not corresponding to relevant passport age.
The uneven diameter and shape of the seminiferous tubules are noted.
Some tubules are curved, compressed, and have a slit-shaped lumen,
whereas the others appear to have an expanded lumen.
Stroma volume is enlarged; the underlying connective tissue elements are frayed.
Staggered, relatively well-preserved, and sharply collapsed seminiferous tubules
are found in the stroma, separated from one another (a, b)
Рисунок 1. Световая микроскопия (окраска гематоксилином
и эозином, микрофуксином, по Ван Гизону, увеличение ×140;
анализ проведен патоморфологом, к.м.н. А.В. Клейном).
Морфология яичек (testes) резко изменена
и не соответствует их паспортному возрасту.
Обращает на себя внимание
неравномерный диаметр семенных канальцев и их форма.
Некоторые канальцы изогнуты, сдавлены и имеют щелевидный просвет,
или, наоборот, просвет их представляется расширенным.
Объем стромы увеличен,
образующие ее соединительнотканные элементы разволокнены.
В строме определяются неравномерно расположенные, отдаленные друг от друга,
относительно сохранные и резко коллабированные семенные канальцы (a, b)
Patients in Group 1 did not undergo analysis of ejaculate and other specialized research methods, as they were unable to provide ejaculate or prostatic fluid, leading to infertility issues. This infertility can serve as an indirect indicator of low sexual maturity in these patients. Consequently, the global hyposexuality observed in patients of Group 1 is likely explained not only by the involvement of the limbic system and hypothalamic nuclei in the pathological process but also by secondary (hypogonadotropic) structural changes in the testes. As indicated above, hyposexuality lacks nosological specificity and cannot be considered a localized symptom of damage to the limbic brain structures.
In 6 out of 10 patients from Group 1 with initial mental disorders who experienced hyposexuality before surgery, after surgical interventions on the temporal lobe, an improvement in their "sexual ability" was noted with no further occurrence of ES. Out of these 6 patients, 4 women got married, 3 had children, and 2 men also got married. However, in 4 patients who were observed before surgery, hyposexuality persisted despite favorable dynamics in ES.
Additionally, hyposexuality was observed to develop after surgical interventions on the temporal lobe in 4 individuals, which was not observed prior to the operation. Among these, 3 patients did not experience ES. Post-surgery, the development of hypersexuality was noted in 4 patients, 2 patients had no ES, and the remaining 2 experienced a significant reduction in their ES.
In Group 2 (n=33), a range of mental disorders were observed, including memory impairments, dysphoria, twilight states of consciousness, personality changes, and varying degrees of dementia. Six patients had severe epileptic psychosis with a prolonged course. In patients whith severe mental disorders, a progression of the disease led to a complete aversion to sexual activity in some cases (5 women), resulting in marital abandonment and divorces. Five patients displayed sexual infantilism, 3 showed hyposexuality, 3 had hypersexuality, and 4 individuals exhibited masturbation tendencies.
Among those in Group 2 who developed TLE after reaching puberty, a broad spectrum of changes in the sexual sphere was observed. The most typical alteration was in the intensity of sexual desire. In some patients, this manifested as hyposexuality, although it was not as widespread as seen in the patients of Group 1. Notably, patients who underwent surgery on the mediobasal structures of the temporal lobe experienced instances of hyposexuality or hypersexuality followed by the subsequent normalization of sexual activity.
In the examination of testicular biopsy fragments from patients in the 2nd group displaying hyposexuality phenomena before surgery, no significant disruptions in the testicular structure were identified. There were instances of hypospermatogenesis, where spermatogenesis was completed, but the number of spermatogenic elements was reduced. The quantity of Leydig cells was normal or slightly increased. In patients with clinical manifestations of hypersexuality, the study of biopsied testicular fragments did not reveal specific morphological patterns in the gonads (Fig. 2). The obtained findings confirm the validity of existing literature data explaining hypersexuality through stimulation of brain limbic system. The results suggest that there are no direct functional connections between the limbic brain region and the testes.
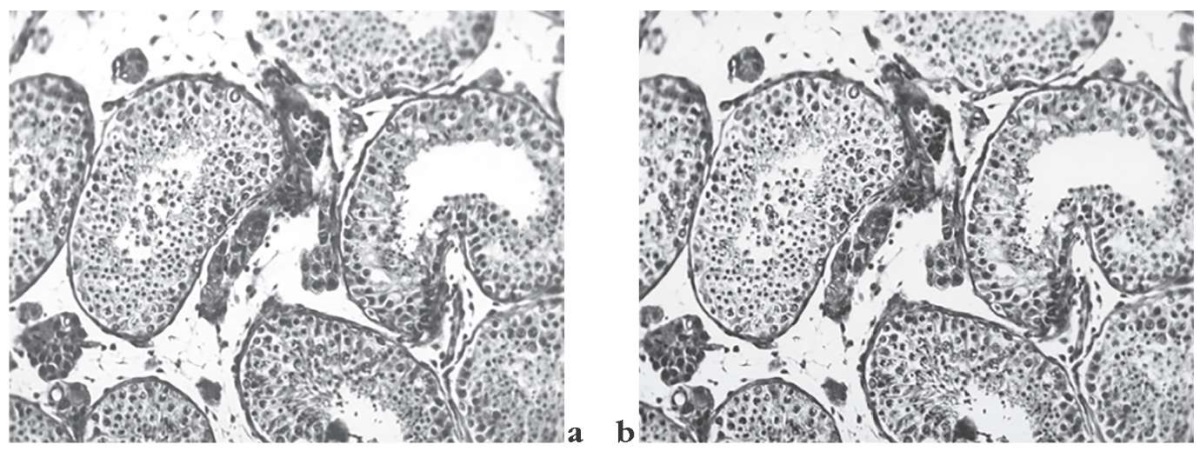
Рисунок 2. Световая микроскопия (окраска гематоксилином
и эозином, микрофуксином, по Ван Гизону, увеличение ×140;
анализ проведен патоморфологом, к.м.н. А.В. Клейном).
Существенные изменения отмечаются в генеративном эпителии.
Стратификационная структура его нарушена.
Так, клетки более раннего периода созревания
(первичные и вторичные сперматоциты),
которые в норме должны находиться в средней зоне эпителиального пласта,
ближе к базальной мембране, зачастую располагаются на поверхности
или даже в просвете канальца. Зрелые сперматиды видны
в ограниченном количестве на отдельных участках (a, b)
Figure 2. Light microscopy (stained with hematoxylin
and eosin, microfuxin, Van Gieson stain, magnification ×140;
the assay was performed by pathomorphologist A.V. Klein, MD, PhD).
The male generative epithelium underwent profound changes,
with its stratified structure being altered.
As a result, cells from an earlier maturation period
(primary and secondary spermatocytes),
which should normally be located in the middle zone of the epithelial layer,
closer to the basement membrane, are frequently found
on the surface or even in the tubule lumen.
Mature spermatids can be seen in small numbers in some areas (a, b)
Upon examining prostatic fluid for the "fern" phenomenon, we observed "scaling" and "fragmentation" phenomena in all patients within this group. These abnormalities normalized after administering choriogonin, indicating their central origin. In the analysis of ejaculate, varying degrees of oligoasteratozoospermia were observed in some patients. Additionally, low fructose levels doubled after choriogonin administration, further supporting the central origin of these disorders.
Considering the structural changes observed in testicular tissue, indicative of secondary (hypogonadotropic) hypogonadism, substitution therapy was administered, yielding positive therapeutic results. This included using a 5% oil solution of testosterone, sustanon 250, high doses of methyltestosterone, choriogonin, Prephyson, and hormone therapy.
Among 5 women with aversion to sexual activity, there was no improvement before surgery, even though 3 of them did not experience ES. In 2 out of 5 women initially classified with
"sexual infantilism," hypersexuality was observed after surgery, manifesting itself in the form of masturbation. However, no changes occurred in 3 patients in this subgroup, despite the complete cessation of ES. In 2 out of 4 patients, cessation of masturbation was noted after surgical interventions on the temporal lobe. Interestingly, the emergence of hypersexuality was observed in 4 individuals following the surgery. As a result, 1 patient had to undergo tubal ligation, although ES stopped after the operation. One patient developed sexual perversions after surgery. Initially, this patient experienced frequent ES during the first year, which later ceased. He stopped engaging in sexual activity after the operation but began to masturbate. The conversations within the family, despite the presence of children, were reduced to sexual topics, often involving cynical expressions.
The discrepancies in symptoms among patients in Group 2 can be better understood when considering studies indicating the existence of a dual regulatory system for sexual processes in the hypothalamus, acting in opposing directions. While the posterior hypothalamus maintains normal excitability of these processes, the anterior hypothalamus has an inhibitory effect. Damage to the anterior hypothalamus, removing this inhibitory effect, can lead to premature puberty, while damage to the posterior hypothalamus delays its onset [21]. There seems to be a distinct functional connection between the limbic brain, the anterior, and the posterior hypothalamus. In patients with hyposexuality, the anterior hypothalamus might be involved in the pathological process due to stimulation from limbic structures, whereas in cases of hypersexuality, the posterior hypothalamus is likely activated, leading to increased sexual desire. This hypothesis is more plausible given that certain structures of the hypothalamus have direct connections with the hippocampus and are interconnected within "motivation systems" [22].
Table 2 shows data on patients' ability to work. It's noteworthy that all patients with severe mental disorders were disabled. Among the children, only 3 out of 8 were able to continue their studies in a regular school setting, while one of them attended a school designated for mentally challenged children.
Таблица 2. Данные по оценке трудоспособности больных (n=82), n (%)
Table 2. Data assessing work capacity (n=82), n (%)
|
Work capacity / Показатель трудоспособности |
Group 1 (mild mental disorders) / 1-я группа (незначительные психические нарушения) |
Group 2 (severe mental disorders) / 2-я группа (выраженные психические нарушения) |
|
Able to work in their chosen profession / Трудоспособен в своей профессии |
4 (8,3) |
– |
|
Able to work, but compelled to engage in less demanding tasks due to illness / Трудоспособен, но вынужден из-за болезни выполнять более легкую работу |
7 (14,5) |
– |
|
Disability group III / III группа инвалидности |
10 (20,8) |
– |
|
Disability group II / II группа инвалидности |
8 (16,6) |
19 (57,5) |
|
Disability group II / I группа инвалидности |
1 (2,0) |
6 (18,1) |
|
Continue school attendance / Продолжают учебу в школе |
15 (31,5) |
3 (9,9) |
|
Terminated education due to illness / Не учатся по болезни |
3 (6,2) |
5 (13,1) |
|
Total / Всего |
48* (100,0) |
33 (100,0) |
Note. * Тhe female patient aged 4.5 years is not included.
Примечание. * Больная в возрасте 4,5 года не представлена в таблице.
Table 3 displays the probable etiological factors observed in the patients from Groups 1 and 2.
Pathology of the perinatal period and childbirth in the mother in the form of epilepsy is given leading importance [22–24]. In our observations, based on the medical history, we were able to identify pregnancy and childbirth-related pathology in 30 (37.6%) patients. It's essential to note that not all patients provided complete obstetric histories, and in 7 cases, the exact etiological factor could not be established.
Table 3. Etiological factors of temporal lobe epilepsy (n=82), n (%)
Таблица 3. Этиологические факторы височной эпилепсии (n=82), n (%)
|
Etiological factor / Этиологический фактор |
Group 1 (mild mental disorders) / 1-я группа (незначительные психические нарушения) |
Group 2 (severe mental disorders) / 2-я группа (выраженные психические нарушения) |
|
Genetic factors / Наследственные факторы |
13* (26,5) |
10** (30,3) |
|
Maternal pathology of pregnancy and delivery / Патология беременности и родов у матери |
14 (28,5) |
9 (27,3) |
|
Severe childhood diseases / Тяжелые заболевания в детском возрасте |
11(22,4) |
4 (12,1) |
|
Traumatic brain injury / Черепно-мозговая травма |
6***(12,2) |
3*** (9,1) |
|
Other etiological factors / Прочие этиологические факторы |
3 (6,1) |
2 (6,1) |
|
Undetermined / Не установлен |
2 (4,8) |
5 (15,2) |
|
Total / Всего |
49 (100,0) |
33 (100,0) |
Note. * One patient recovered from communicable disease in early childhood;
the pathology of pregnancy and delivery was also noted in seven paired patients’ mothers.
** Patients had a variety of severe communicable diseases in early childhood.
*** In addition to traumatic brain injury,
one of the patients had a severe communicable disease.
Примечание. * Один больной в раннем детстве
дополнительно перенес инфекционное заболевание;
в 7 случаях была также отмечена патология беременности и родов у матери.
** В раннем детстве имели различные инфекционные заболевания
с тяжелым течением.
*** Один из этих больных кроме черепно-мозговой травмы
также перенес тяжелое инфекционное заболевание.
Obstetric and gynecological anamnesis included: attempts to terminate pregnancy (2 patients), uterine prolapse (2 patients), uterine bleeding (2 patients), severe preeclampsia (4 patients). Twins were born in 2 patients, premature birth occurred in 3 women, large fetus delivery – in 3 women, asphyxia of newborns took place in 9 cases.
The presence of a hereditary burden was observed in 23 patients, as indicated in Table 4. The influence of genetic factors in the development of epilepsy has been emphasized by several authors [5][19][23][24]. They found a 1.5-fold higher prevalence of epilepsy in TLE relatives compared to non-localized forms of epilepsy. However, it's important to note that hereditary factors only contribute to a child's predisposition to epilepsy. Genetic factors play a significant role in the genesis of epilepsy and hold substantial importance, as confirmed by the surgical treatment outcomes of TLE patients.
Table 4. Hereditary burden in relatives
of patients with temporal lobe epilepsy (n=23), n (%)
Таблица 4. Наследственная отягощенность
у родственников больных височной эпилепсией (n=23), n (%)
|
Type of hereditary burden / Вид наследственной отягощенности |
Males / Мужчины |
Females / Женщины |
Total / Всего |
|
Epilepsy / Эпилепсия |
7 (70) |
3 (23,2) |
10 |
|
Epileptic psychopathy / Эпилептическая психопатия |
2 (20) |
1 (7,6) |
3 |
|
Periodic alcoholism / Запойный алкоголизм |
1 (10) |
2 (15,3) |
3 |
|
Somnambulism / Сомнамбулизм |
– |
1 (7,6) |
1 |
|
Enuresis / Энурез |
– |
1(7,6) |
1 |
|
Migraine / Мигрень |
1 (10) |
2 (15,3) |
2 |
|
Mental illnesses / Психические заболевания |
– |
2 (15,3) |
2 |
|
Congenital deaf-mutism / Врожденная глухонемота |
– |
1 (7,6) |
1 |
|
Total / Всего |
10 (100) |
13 (100) |
23 |
The hereditary burden is particularly notable in TLE patients who also exhibit severe mental disorders; this was observed in one-third of the patients. A particularly unfavorable course was observed in 6 patients from Group 2, where a combination of two etiological factors was present (Table 5).
Table 5. Etiological factors in temporal lobe epilepsy patients
operated at the age of 5–14 years old (n=24), n
Таблица 5. Этиологические факторы у больных височной эпилепсией,
оперированных в возрасте 5–14 лет (n=24), n
|
Etiological factor / Этиологический фактор |
Patient age at surgery, years / Возраст в момент операции, лет |
Total / Всего |
||
|
0–5 |
6–10 |
11–15 |
||
|
Congenital factors / Наследственные факторы |
– |
2 |
4 |
6* |
|
Maternal pathology of pregnancy and delivery / Патология беременности и родов у матери |
1 |
2 |
7 |
10 |
|
Severe infections in early childhood / Тяжелые инфекционные заболевания в детском возрасте |
– |
– |
5 |
5 |
|
Traumatic brain injury / Черепно-мозговая травма |
– |
– |
1 |
1 |
|
Undetermined / Не установлен |
– |
– |
2 |
2 |
|
Total / Всего |
1 |
4 |
19 |
24 |
Note. * The pathology of pregnancy and delivery
was also noted in 5 of paired patients’ mothers.
Примечание. * В 5 случаях также отмечена
патология беременности и родов у матери.
Further discussion of the probable etiological factors in children who underwent surgery between the ages of 5 and 14 is necessary. As indicated in Table 5, among the patients operated on during childhood, the primary leading etiological factor was perinatal pathology. Additionally, 5 patients in this group had a history of severe infections, including measles, chickenpox, whooping cough, and scarlet fever. It's important to note that all the examined patients in this group experienced frequent ES for an extended period before undergoing surgical treatment, with the frequency ranging from 5 to 8 or more seizures per month.
The use of antiepileptic drugs (AEDs) over an extended period failed to yield the desired effect. The duration of the disease from the onset of regular seizures varies among the patients. Among the individuals, 18 experienced the initial appearance of generalized convulsive paroxysms before the age of 10 years, followed by a subsequent period of relative stability lasting 4 to 10 years. Two patients had status epilepticus as their first manifestation, while 5 had febrile seizures, and 4 displayed a focal component in their seizures during that period.
The duration of the disease at the time of surgery is shown in Table 6. As can be seen, there is a significant variation in the duration of the disease from the onset of regular seizures. Surgical treatment was also administered after a considerable period, with interventions conducted as early as 3 years after the commencement of regular ES, and in cases where no effect was observed from the systematic use of AEDs, the surgery was performed after 2 years.
Table 6. Patient distribution by disease duration at the time of surgery (n=82), n (%)
Таблица 6. Распределение больных
по длительности заболевания к моменту операции (n=82), n (%)
|
Disease duration / Длительность заболевания |
Group 1 (mild mental disorders) / 1-я группа (незначительные психические нарушения) |
Group 2 (severe mental disorders) / 2-я группа (выраженные психические нарушения) |
|
3–5 years / 3–5 лет |
17 (34,6) |
6 (18,1) |
|
6–10 years / 6–10 лет |
18 (36,7) |
11 (33,3) |
|
11–15 years / 11–15 лет |
11 (22,4) |
7 (21,2) |
|
16–20 years / 16–20 лет |
2 (4,4) |
8 (24,2) |
|
21–25 years / 21–25 лет |
– |
1 (3,1) |
|
26–30 years / 26–30 лет |
– |
– |
|
>30 years / Более 30 лет |
1 (2,1) |
– |
|
Total / Всего |
49 (100,0) |
33 (100,0) |
The characteristics of the paroxysmal syndrome play a crucial role in the localization diagnosis of the epileptogenic focus within the temporal lobe. Paroxysmal syndrome is comprised of distinct phases, including prodromal phenomena, aura, the seizure period, and the post-seizure state.
The least common among these are prodromal phenomena observed in 15 patients, indicating the imminent onset of seizures. These prodromal signs typically entail a low mood background, vague anxious anticipation, and accompanying autonomic dysfunctions such as sleep disturbances, thirst, anorexia, and migraine headaches. It's noteworthy that individuals experiencing these prodromal phenomena face a significantly higher risk of developing psychological issues, such as depression, anxiety, and psychosis, compared to the general population [21][25][26].
The types of surgical interventions and the side of the operation performed are detailed in Tables 7, 8.
Hence, TLE patients tend to experience sexual disharmony, with hyposexuality being the predominant issue. In cases where the disease onset occurs during the first decade of life, we observed subsequent development of sexual infantilism. Our data indicate that hypersexuality and sexual perversions are most commonly associated with patients who have severe mental disorders.
In the group of patients with pronounced psychological issues, a small portion experienced regression of SDs after surgical interventions on the temporal lobe and removal of the epileptogenic focus. Positive outcomes were noted in patients who exhibited hypersexuality before the operation, and this symptom subsided along with the cessation of ES.
Table 7. Types of surgical intervention in patients with temporal lobe epilepsy (n=82)
Таблица 7. Виды оперативных вмешательств у больных височной эпилепсией (n=82)
|
Type of surgical intervention / Вид оперативного вмешательства |
Number of surgeries, n / Количество операций, n |
|
Subpial resection of the temporal cortex / Субпиальная резекция коры височной доли |
2 |
|
Anterior temporal lobectomy with resection of mediobasal structures (amygdaloid nucleus and hippocampus) / Передняя височная лобэктомия с резекцией медиобазальных структур (миндалевидного ядра и гиппокампа) |
53 |
|
Extended temporal lobectomy with resection of the insular cortex and frontal operculum / Расширенная височная лобэктомия с резекцией коры островка и лобной покрышки |
7 |
|
Combined stereotaxic destruction of ipsilateral temporal lobe focus with contralateral anterior temporal lobectomy / Комбинированная стереотаксическая деструкция очага височной доли на одной стороне с передневисочной лобэктомией на другой стороне |
2 |
|
Diagnostic stereotaxic operations with intracerebral electrode insertion / Диагностические стереотаксические операции с интрацеребральным введением электродов |
18 |
Table 8. Anatomical sides for surgical intervention
in patients with temporal lobe epilepsy (n=82), n
Таблица 8. Стороны оперативного вмешательства
у больных височной эпилепсией (n=82), n
|
Anatomical side for surgical intervention / Сторона оперативного вмешательства |
Group 1 (mild mental disorders) / 1-я группа (незначительные психические нарушения) |
Group 2 (severe mental disorders) / 2-я группа (выраженные психические нарушения) |
|
Left / Левая |
22 |
11 |
|
Right / Правая |
27 |
22 |
|
Total / Всего |
49 |
33 |
According to our data, SDs in patients with medio-basal temporal lobe lesions are quite common – in 63.3% of cases. Sexual history, objective examination data, and the results of special research methods suggest that sexual disorders in TLE patients are associated with the involvement of the hypothalamic nuclei in the process, which, in turn, causes pathological shifts in the gonads.
1. Maclean P.D. The limbic system and its hippocampal formation; studies in animals and their possible application to man. J Neurosurg. 1954; 11 (1): 29–44. https://doi.org/10.3171/jns.1954.11.1.0029.
2. Blumer D., Wolker E. Sexual behavior in temporal lobe epilepsy. A study of the effects of temporal lobectomy on sexual behavior. Arch Neurol. 1967; 16 (1): 37–43. https://doi.org/10.1001/archneur.1967.00470190041005.
3. Wolker A.E. Recent memory impairment in unilateral temporal lesions. AMA Arch Neurol Psychiatry. 1957; 78 (6): 543–52. https://doi.org/10.1001/archneurpsyc.1957.02330420003001.
4. Khait N.Z., Khait S.E. Sexual pathology in men with temporal lobe epilepsy. In: Temporal lobe epilepsy. Materials of the All-Russian Conference of Neuropathologists, Psychiatrists and Neurosurgeons. Tyumen; 1970: 122–4 (in Russ.).
5. Karlov V.A. Epilepsy in children and adult women and men: a guide for doctors. 1st ed. Moscow: Meditsina; 2010: 720 pp.
6. Gastaut H., Morin G., Lesevre N. Behavior of psychomotor epileptics between seizures; disorders of general activity and sociability. Ann Med Psychol (Paris). 1955; 113 (1): 1–27 (in French).
7. Klüver H., Bucy P.C. An analysis of certain effects of bilateral temporal lobectomy in the rhesus monkey, with special reference to “psychic blindness”. J Psychol. 1938; 5 (1): 33–54. https://doi.org/10.1080/00223980.1938.9917551.
8. Pilleri G. The Klüver–Bucy syndrome in man. A clinico-anatomical contribution to the function of the medial temporal lobe structures. Psychiatr Neurol (Basel). 1966; 152 (2): 65–103.
9. Poeck K. The Klüver–Bucy syndrome in man. In: Frederiks J.A. (Ed.) Handbook of clinical neurology. New York: Elsevier; 1985: 257–63.
10. Janati A. Klüver–Bucy syndrome in Huntington’s chorea. J Nerv Men Dis. 1985; 173 (10): 632–5. https://doi.org/10.1097/00005053198510000-00010.
11. Wood C.D. Behavioral changes following discrete lesions of temporal lobe structures. Neurology. 1958; 8: 215–20.
12. Maclean P.D. The limbic system (“visceral brain”) and emotional behavior. AMA Arch Neurol Psychiatry. 1955; 73 (2): 130–4. https://doi.org/10.1001/archneurpsyc.1955.02330080008004.
13. Yamada T., Greer M.A. The effect of bilateral ablation of the amygdala on endocrine function in the rat. Endocrinology. 1960; 66: 565–74. https://doi.org/10.1210/endo-66-4-565.
14. Ado A.D., Ishimova L.M. (Eds.) Pathological physiology. 2nd ed. Moscow: Medicine; 1980: 520 pp. (in Russ.).
15. Popov S.V. Erectile dysfunction in brain diseases. Russian Medical Journal. 2014; 22 (4): 272 (in Russ.).
16. Astaf’eva L.I., Zhukov O.B., Kadashev B.A., et al. Reproductive disorders and preservation of fertility in males with benign and malignant brain tumors. Problems of Neurosurgery named after N.N. Burdenko. 2019; 83 (2): 59–65 (in Russ.). https://doi.org/10.17116/neiro20198302159.
17. Zambrzhitskiy I.A. Limbic region of the large brain. Мoscow: Meditsina; 1972: 117–28 (in Russ.).
18. Leeds N.E., Kieffer S.A. Evolution of diagnostic neuroradiology from 1904 to 1999. Radiology. 2000; 217 (2): 309–18. https://doi.org/10.1148/radiology.217.2.r00nv45309.
19. Shefer D.G. General issues of the clinic, diagnosis and surgical treatment of temporal lobe epilepsy. In: Temporal lobe epilepsy. Materials of the All-Russian Conference of Neuropathologists, Psychiatrists and Neurosurgeons. Tyumen; 1970: 3–7 (in Russ.).
20. Zemskaya A.G. Features of the clinical course of epilepsy and postnatal trauma and surgical tactics. In: Epilepsy. Proceedings of the Interregional Conference of Neuropathologists, Neurosurgeons and Psychiatrists of Western Siberia and the Urals. Omsk; 1967: 166–9 (in Russ.).
21. Shagina V.N., Blokhina I.I., Serov I.S. Conditions developing with damage to the hypothalamus. Molodoy uchenyy / Young Scientist. 2019; 36: 28–30 (in Russ.).
22. Krylov V.V. Surgery of epilepsy. Moscow: ABV-press; 2019: 408 pp. (in Russ.).
23. Davidenkov S.N. Epileptic seizures in temporal lobe lesion. In: Davidenkov S.N. Clinical lectures on nervous diseases. Vol. 1. Leningrad: Medgiz; 1952: 5–23 (in Russ.).
24. Rathore C., Radhakrishnan K. Epidemiology of epilepsy surgery in India. Neurol India. 2017; 65 (Suppl.): S52–9. https://doi. org/10.4103/neuroindia.NI_924_16.
25. Charyton C., Elliott J.O., Lu B., Moore J.L. The impact of social support on health related quality of life in persons with epilepsy. Epilepsy Behav. 2009; 16 (4): 640–5. https://doi.org/10.1016/j.yebeh.2009.09.011.
26. Gellhorn E., Loofbourrow G.N. Emotions and emotional disorders. A neurophysiological study. New York, London: Harper and Low; 1963: 90 pp.
David G. Shefer – Dr. Med. Sc., Professor, Chief of Chair of Nervous Diseases and Neurosurgery
Yekaterinburg
Alexander S. Shershever – Dr. Med. Sc., Professor, Neurosurgeon, Neurologist, Deputy Chief Physician for Science
Yekaterinburg
Valeriy B. Boreyko – MD, PhD, Psychiatrist
Yekaterinburg
Aleksey V. Klein – MD, PhD, Pathomorphologist
Yekaterinburg
Elena V. Sorokova – MD, PhD, Neurologist, Epileptologist, Chief Physician
Yekaterinburg
Shefer D.G., Shershever A.S., Boreyko V.B., Klein A.V., Sorokova E.V. Sexual disorders among temporal lobe epilepsy patients preand post-surgery. Epilepsy and paroxysmal conditions. 2023;15(3):210–221. https://doi.org/10.17749/2077-8333/epi.par.con.2023.148

117042, Moscow, Chechersky passage, 24
Tel.: +7(495)6495495
e-mail: info@irbis-1.ru



































